Physician's Notebooks 6 - http://physiciansnotebook.blogspot.com - See Homepage
Update 20 Aug. 2021
Update 20 Aug. 2021
6. Coronary Artery Disease & Coronary Heart Disease (CAD & CHD are closely related; CAD is primary disease in the walls of the coronary arteries that supply the heart muscle; CHD is a result of CAD or other conditions that cause heart disease. The CHD (Coronary Heart Disease) can also be due to diseases or accident without CAD, as in infection or trauma or tumor of the coronary arteries.)
(Use a loupe to inspect; also Google the coronary arteries)
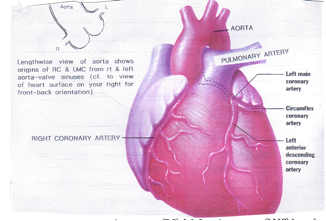
The coronary arteries arise as right coronary (RC) & left main coronary (LMC) off aorta at its root.
Your heart is a muscle pouch and needs oxygen (O2) carried to its tissues loosely attached to hemoglobin (Hgb) in red blood cells (normally in artery blood the Hgb is 98% saturated with O2) and, to a much lesser extent dissolved in blood plasma (0.3% O2). Blood also carries, in its fluid plasma, glucose and fatty acids that, with the O2, produce energy for the heart to beat.
An obstruction in a coronary artery can lead to a sharp reduction in blood flow and reduce oxygen and nutrients to heart muscle, resulting first in angina heart pain and, if unrelieved, in acute myocardial infarct(ion; AMI), which may lead to sudden death or, if survival occurs, it may leave a victim with a failing heart.
Coronary Artery Cholesterol Plaque Development – 4 Stages

1) Healthy state at birth: blood flows unobstructed.
2) In childhood, because of eating too many calories a day, early cholesterol plaque in lining of artery may form fatty streaks, and then the rough lining wall attracts blood platelets on it and the platelets release chemicals that attract more platelets to form a plaque that starts to narrow the artery.
3) In the adult, the platelet-cholesterol plaque builds up, partly obstructing blood flow. If more than 75% obstructed, it causes chest pain on exertion ("angina").
4) Growth pressure or external trauma or infection causes plaque to break open and exposes fatty cholesterol content to fluid blood plasma, causing blood to clot and obstruct the artery. If the clot is not quickly dissolved, the heart muscle supplied by the artery develops an infarct, and if the infarct gets too big, you may die too.
The key to prevention and successful intervention in Coronary Artery Disease, comes from understanding how it develops, identifying factors involved, and preventing progression.
We also need to know about final stage – the Acute Myocardial Infarct (AMI) – in order to intervene to limit damage and prevent death.
Most of us are born with perfect coronary arteries. But at end stage CAD, some of us die from AMI with one or more obstructed coronary arteries.
Atherosclerosis (fatty plaque obstruction of arteries) stages are: At birth, normal; in childhood, fatty streak in artery wall; in young adult progressing from streak to plaque; in middle & old age the plaque cracks under minor trauma or infection, and clot forms final blockage forcing an AMI with sudden or late premature death or heart failure.
Focus on the plaque: a rough spot in artery wall, like spot of rust in a pipe. It starts a vicious cycle: plaque attracts platelets, each platelet attracts more platelets and makes plaque rougher and narrows artery further; at next stage the surface of plaque cracks due to trauma (high blood pressure pulse, blow to chest, excess X-ray to chest, touch of catheter during heart test, or infection from other parts of body like from the throat or the teeth), causes inflammation in artery, and clot to form over the plaque. If in major coronary artery, the blockage deprives large area of heart muscle from getting oxygen. If blockage is not reopened quickly (minutes to hour), it destroys tissue by forming an Acute Myocardial Infarct (AMI) and causes pain, and heart failure or death may follow.
Preventive advice
1) Cholesterol (LDL-C, the important cholesterol for heart disease) in blood is a modifiable risk factor from moment of birth. Work to attain low LDL cholesterol by healthy eating and by using Statin lower-cholesterol pills.
2) Wear & tear on artery: High blood pressure pulsations are a risk factor in CAD. Repeated overstretching of artery wall with each high BP heartbeat will speed tearing and worsen plaque/platelet-cycle. And a too high BP gets transmitted back to the heart's left ventricle, stiffening it and slowing blood flow to heart muscle. High BP especially with a relatively rapid resting heartbeat (RHB) also ups the heart muscle demand for oxygen, requiring a higher rate of coronary artery blood flow. So an aggressive attitude toward hypertension – for definitive BP testing by proper technique (biceps wrap-around by physician using stethoscope soundings technique)— and also paying attention to keeping your RHB low by physician prescribed beta-blocker med, using top medical team and not being satisfied with other than best lowering of BP – is a must for healthy longevity CAD prevention. Other bad wear and tear factors are intravenous drug shooting-up (damage from particle and infection), cocaine and amphetamines (constricts coronary arteries); also, jogging and jolting body contact sport (shearing injury to plaque from jolt).
3) Keep blood well diluted with water. The plating out of cholesterol in artery is a dynamic moment-to-moment effect that depends on concentration of cholesterol in fluid blood and goes on for life. It is not completely one-way, because when blood LDL-Cholesterol falls sharply, some cholesterol in fatty streak or plaque is washed back into the blood, decreasing the size of the plaque. So the more you dilute your blood fluid, the better for your good health. Also, dilution mildly inhibits blood clotting, a good preventive against the acute MI. No matter your blood test's Total and LDL Cholesterol, drinking more water lowers it. The old dilute & flush water treatment! Costs nothing, is harmless, and stops CAD.
4) Daily Anti Platelet-Aggregation Medication. (Usually by taking as low as a quarter 325 mg aspirin a day).
5) Several times daily 30- to 60-min. lie-flat repose (not deep sleep).
7) Keep low resting heart rate 55 to 65 per minute by no unnecessary heavy effort and practicing calm meditation; and use low dose beta-blocker medication often with ACE-Inhibitor.
The Angina Syndrome: Recognizing angina is key to prevent death from it. Angina is caused by making the heart work extra (Walking up steep hill, facing cold wind, walking up stair, doing sex) or by strong emotion, or after eating, or by high blood pressure especially with rapid heart rate, or bad dream. Or even heavy clothing. Angina is centered in chest, deep to or just below breastbone and may radiate to left shoulder and wing bone and down inner aspect of arm to 3rd, 4th and 5th finger or up to neck and jaw. Quality varies from “pressing” pain, e.g., “Someone sitting on my chest and I can’t breath” to “like butterfly in my breast,” to mild, irritating pain in left shoulder, scapula (collar bone) or wrist. It has rapid onset in relation to inciting incident and sufferer stops and gets relief sitting or lying quietly. It recurs the same way and with same quality but may worsen over time. It may at first be blamed on heartburn, indigestion or acidity, or on gastric-esophageal reflux (GERD). That or other stomach or digestive symptoms, however, are not brought on by exertion or emotion.
Treatment Relief: Angina occurs when localized heart muscle demand for oxygen outstrips its blood supply. Rapidly relieved either by increasing oxygen (breathing 100% O2) or increasing blood supply (nitroglycerin widens coronary artery) or reducing work of heart from slowing the heartbeat (rest from exertion, beta blocker or calcium channel blocker meds).
Stage where you have no symptom yet are at high risk requires your knowledge and actions. If we take the stage without symptom even under stressful exercising condition, what test is best? The blood tests and resting EKG help you determine your risk factors but they cannot answer: Do I have significant CAD that I need now to do something about? The best screening is stress EKG step test a.k.a. Duke Treadmill Test.
When to get the test? If you have risk factors or feel neurotic about having heart disease get it now. If the test is normal, it should relieve your neurosis. If abnormal, it will lead you in the direction of good preventive CAD care.
Once you are Class I (Canadian Cardiovascular Society Functional Classification) CAD ("Stable angina", definition - ordinary activity does not cause angina but positive symptoms on exertion or positive Stress test) you need to follow a preventive program. It means to get the LDL-C to 60 mg% or lower by eating right and taking a statin-lowering cholesterol medicine; to get the BP below 130/80 with an RHB between 55 and 65 by lifestyle and, if necessary, medication; and to get your blood into proper clotting state by taking low dose aspirin, lots of water and doing good functional exercise. And do not forget weight as body mass index: strive to get your BMI down to 20 or lower before age 60. If you are getting your LDL cholesterol down, you will need to test at intervals until you reach your goal. Similarly for getting HDL cholesterol up to healthy level.
When to get the test? If you have risk factors or feel neurotic about having heart disease get it now. If the test is normal, it should relieve your neurosis. If abnormal, it will lead you in the direction of good preventive CAD care.
Once you are Class I (Canadian Cardiovascular Society Functional Classification) CAD ("Stable angina", definition - ordinary activity does not cause angina but positive symptoms on exertion or positive Stress test) you need to follow a preventive program. It means to get the LDL-C to 60 mg% or lower by eating right and taking a statin-lowering cholesterol medicine; to get the BP below 130/80 with an RHB between 55 and 65 by lifestyle and, if necessary, medication; and to get your blood into proper clotting state by taking low dose aspirin, lots of water and doing good functional exercise. And do not forget weight as body mass index: strive to get your BMI down to 20 or lower before age 60. If you are getting your LDL cholesterol down, you will need to test at intervals until you reach your goal. Similarly for getting HDL cholesterol up to healthy level.
Classes II and III (Slight or marked limits of activity aka Stable Angina)
With stable angina you can assume you have 50 or more% narrowing of coronary arteries and are at risk for Myocardial Infarction. Do test to identify the coronary narrowing and reverse it. The key test is a Coronary Computed Tomography Angiography (CTA; Magnetic Resonance Imaging Angiography may soon be better but presently is a little less accurate). The CTA will either show coronary artery narrowing(s) that can be treated by angioplasty/stenting or by coronary artery bypass surgery or it will show that surgical or inter-ventional treatment is unwise. In the former case the CTA should be followed by catheter coronary artery angiography x-rays with dye during which angioplasty/stenting may be done or which may set up the patient for coronary artery bypass surgery. Where angioplasty or bypass is unwise, aggressive medical treatment with lipid lowering/antihypertensive/ACE inhibitor/beta blocker drug and nitrates for symptoms may be called for.
Class V:Unstable Angina (Discomfort even at rest) or Myocardial Infarction
Acute Myocardial Infarct(ion), the death of area of heart muscle due to blockage of feeding artery, is the feared finale of CAD. The effect of infarction can vary from none, when very small area of total muscle is affected, to death from pump failure when it involves more than 40% of heart muscle. So the more an infarct size can be limited, the better chance for good outcome. If you get a myocardial infarct, you must immediately get in hospital.
Why the infarct? The MI final stage occurs because blood clot forms in artery that supplies infarct segment. Red blood cell hemoglobin gives most of the oxygen excepting the oxygen that is 0.3% physically dissolved in blood plasma if you breathe room air with 21% O2. (Plasma oxygen can be increased 7 times by breathing pure oxygen)
Why the clot? It forms because a segment of artery has been narrowed and roughened in its lining by cholesterol plaque. But narrowing is not enough. Final event is crack and tear of cap that causes the cholesterol inside the plaque to come into contact with the blood flowing in the artery. Two processes are going on: 1) long-term coronary artery wall plaque formation with narrowing and 2) sudden tearing or cracking of plaque cap, which causes clot blockage. Preventing plaque formation and growth is a lifetime program but opening up a clot blockage is another story. Here, time (minute to 6 hours from instant of clot blockage) of intervention makes difference between dying and living or, if life continues, between a healthy and a damaged heart.
Why the tearing or cracking? As the plaque builds-up it becomes like a pimple of inner lining of artery, and its inner mass bulges the overlying wall into the artery. The content is fatty, separated from the blood flow in artery only by thin cap of lining. Continued growth of plaque stretches cap. As stretching becomes too much, the cap tears and rips open. This tearing is made easier (and hence comes earlier) by conditions that wear down the cap: high blood pressure pulsations, infection, inflammation, even sudden jolt (as in jogging or blow to chest). And then the plaque substance comes into contact with flowing blood in artery. Immediately, platelets are activated to aggregate and start blood clotting. Once the clot blocks the artery, the part of the artery forward of the clot becomes stagnant and the clot propagates in its direction, blocking other feeding branches and worsening the infarct.
If the coronary artery clot is not dissolved ASAP up to 3 hours, a lesser or greater size Acute Myocardial Infarct (AMI) develops. (Size depends on completeness of deprivation of blood flow, the oxygen demand of muscle based on heart rate and blood pressure, and amount of oxygen physically dissolved in tissue fluid)
Time counts – In actual intervention, when clot is dissolved or removed within 1 hour after onset of chest pain, the AMI is headed off.
Time counts – In actual intervention, when clot is dissolved or removed within 1 hour after onset of chest pain, the AMI is headed off.
The several hours after the initial artery blockage and the first sign of AMI are an unstable period of infarct enlargement because of propagation of clot into other branches of artery.
Why does one die with AMI? Some die in the first hours from isolated arrhythmia (fibrillation, heart block). Tragically, it may be a small infarct which – had it not been in the one crucial spot – would have caused no symptom and left no after-effect. “A heart too good to die!” is the meaningful phrase. Thus the importance of anti-arrhythmic drug (beta-blocker already being taken or available at home). Later deaths (hour to day) are due to increasing size of the infarct by spreading inflammation and artery block causing progressive heart failure. Thus, the full dose (325 mg) aspirin at first indication of MI and high-flow 100% oxygen inhalation.
To protect your heart from MI needs commitment, forethought, and preparation. Follows the 4-point program.
1. Rapid Self-Diagnosis. Minute counts! Heart injury starts after several minutes coronary blockage. Dissolving clot (by coronary artery catheter thrombolysis ) is effective but less and less as time goes by, up to 6 hours from onset of blockage. Since you will not be in medical hands at onset of symptom, your initial behavior will be key to saving heart muscle and maybe your life by making every second count in heart-protective and coronary-care-corrective action. When chest pain hits – no matter age, sex, inciting circumstance or other risk factor – Acute MI should pop-up in mind. Action button should be pushed by pain in mid-chest at the start of any physical activity (typically walking uphill against cold wind or starting sexual intercourse) which is crushing, squeezing, pressing, expanding, or aching, and especially if it radiates to left shoulder and down inner arm, or to jaw, and most especially if accompanied by nausea or faintness. The key is chest ache. Rapid intervention can be curative so speed, speed, speed!
2. Call ambulance you know (by having checked ahead of time before the episode of pain) will have paramedic prepared to deal with MI and bring you to medical center that can do rapid coronary artery thrombolysis and/or balloon angioplasty/stenting.
3. Chew 1 adult aspirin (325 mg, because this dose has the needed anti-inflammation not obtainable by usual low dose, and chewing it speeds absorption into blood). Then start breathing 100% oxygen in well-fitted, firmly applied mask. (Anyone at risk should have a small canister of oxygen with breathing apparatus.) While waiting for ambulance, lie down with legs elevated from the hips and your arms, when not in use, held above head. (Infuses needed extra blood volume from extremities to heart and brain using gravity and protects brain from low blood pressure.) Breathe oxygen 15 to 20 breathes per min. Have a beta blocker pill available (by doctor Rx, stored at home, if you determine you are at risk) and chew it to protect heart muscle by its heart rate slowing effect.
4. Finally, be tranquil despite natural anxiety. Having taken this reading seriously and made appropriate preparation, and acted on it, you will have every reason to feel tranquil: The oxygen, the aspirin, the beta blocker will, within minute, be protecting your heart and relieving pain; the reclining body position will be giving heart and brain max oxygen in blood as well as reducing heart work; and the first-of-all call for pre-checked paramedic ambulance will give assurance that best help is speedily on way to take you to best hospital where coronary intervention can remove the block. (Yes, it May sound Utopian but the model is god!) Then, ‘leave the driving to others’, first (actual) to the paramedics, next (metaphoric) to ER personnel and cardiology team at medical center.
End of Chapter. To read next now, click 6.7 Cardiac Meds & Interventions like Stents and ...
1 comment:
lypo spheric vitamin c can be used by the whole family. Lypo-Spheric Vitamin C is indicated for cold, chronic sinusitis, viral or bacterial infections. Take two sachets in a small cup/glass of water every 4 hours for the first day Reduce to one sachet morning and night the second day if symptoms are improving.
Post a Comment